Key points
- A mastectomy is necessary for some patients due to tumour size, multifocality, widespread DCIS or if radiation treatment is contraindicated.
- There are four types of mastectomy: simple mastectomy, modified radical mastectomy, skin-sparing mastectomy and nipple-sparing mastectomy.
- Radiation to the chest wall may be recommended post-mastectomy.
Mastectomy
A mastectomy (surgical removal of the whole breast) may be clinically indicated when:
- the tumour is large, or large relative to breast size
- multifocal tumours - DCIS is widespread
- tumour is locally advanced - tumours with skin or chest wall involvement
- the patient is unable or unwilling to undergo radiation treatment that is standard treatment following a partial mastectomy.
- the patient has a genetic predisposition to breast cancer.
With modern oncoplastic techniques, many cases that were previously considered only appropriate for mastectomy, may now be offered breast conservation.
Patients may also choose to have a mastectomy. Often this is based on fear of local recurrence (although local recurrence rates are very low with modern BCS and radiotherapy).
There are four types of mastectomy:
Simple mastectomy
The whole breast is removed along with the nipple, areola and an area of surrounding skin. A sentinel lymph node biopsy is almost always performed to investigate the presence of cancer cells in the axilla.
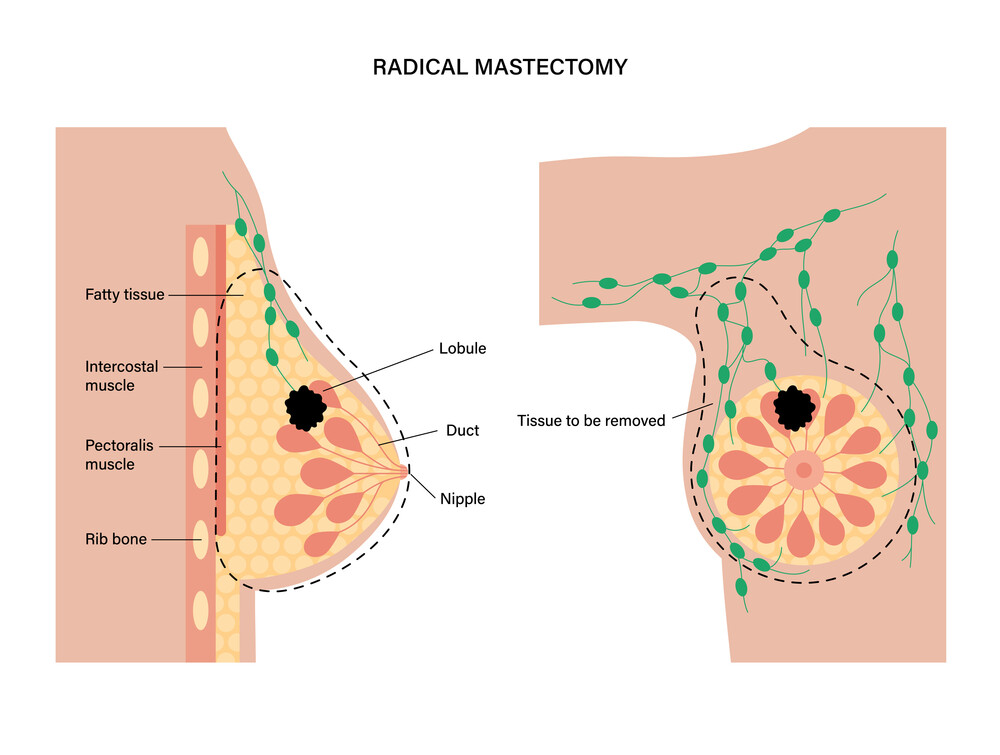
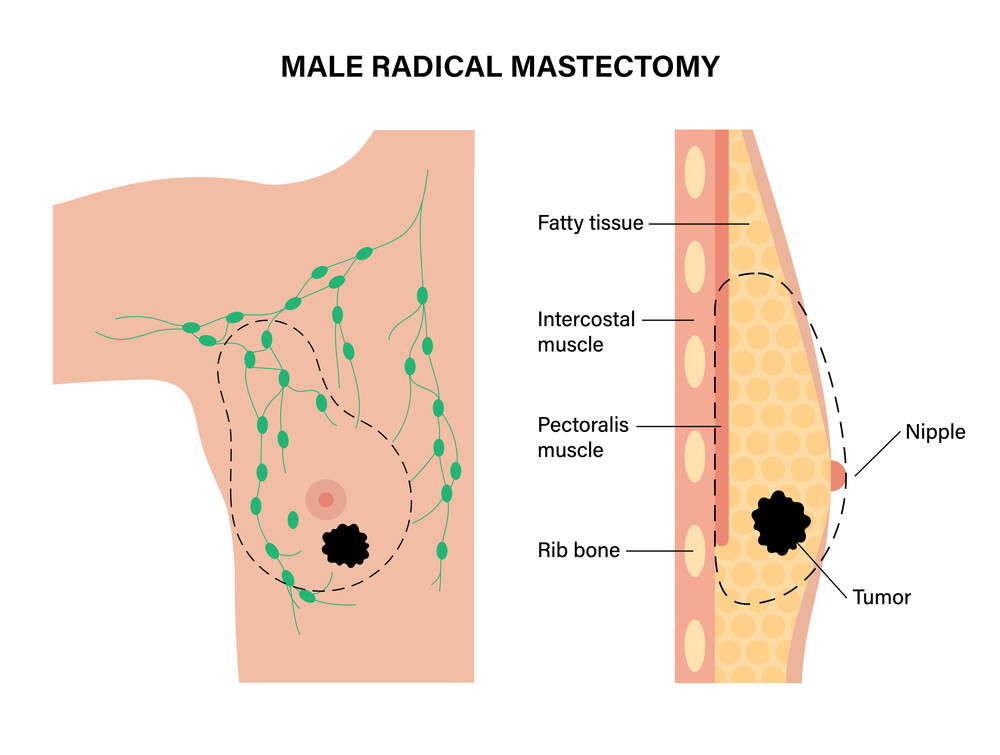
Modified radical mastectomy
This is the same as a simple mastectomy, with the addition of axillary node dissection, usually up to level two.
Skin-sparing mastectomy
Skin-sparing mastectomy
The whole breast, nipple and areola are removed, but more surrounding skin is preserved to facilitate immediate breast reconstruction. Sentinel node biopsy or axillary node dissection is performed as appropriate.
Nipple-sparing mastectomy
The whole breast is removed but the nipple and areola are preserved for immediate reconstruction. Sentinel node biopsy or axillary node dissection are performed as clinically indicated.
Post-surgery, patients may be discharged with a drain in situ. Patient is referred to the district nurse team and the drain is removed once fluid output is minimal.
A mastectomy minimises the need for radiation therapy post-surgery. However, radiation to the chest wall may be recommended if:
- the tumour is large, has four or more positive lymph nodes, has positive margins or other high-risk features; or
- one to three lymph nodes are involved and there are other potentially high-risk features (e.g. grade 3, triple negative breast cancer, lymphovascular space invasion).
Some patients may opt to have breast reconstruction post-mastectomy.