Key points
- Autologous reconstruction uses a patient’s own tissue for breast reconstruction.
- Autologous reconstruction procedures include pedicled flaps, microvascular flaps and perforator flaps.
Autologous reconstruction
Autologous reconstruction uses a woman’s own tissue and/or muscle to reconstruct the breast. Autologous flaps use natural tissue, resulting in a breast that looks and feels more natural than an implant. The breast will change naturally with weight fluctuations and ageing, which helps maintain breast symmetry.
Immediate reconstruction (prior to post-mastectomy radiation) is more likely to be an option with autologous reconstruction than with implant reconstruction.
Considerations
Factors to consider prior to autologous reconstruction include:
- Complexity and length of surgery with a longer recovery time
- Scarring at donor site and breast
- possible loss of strength due to muscle defect (DIEP) if muscle used
- risk of hernia with abdominal flaps
- seroma development
- risk of partial or complete flap failure.
There are multiple procedure options for autologous breast reconstruction.
The DIEP (Deep Inferior Epigastric artery Perforator) flap uses tissue from the same abdominal area as the TRAM flat, but doesn’t use muscle. As such, there is minimal loss of abdominal strength and faster recovery compared to a pedicled TRAM flap.
Free TRAM flap uses the same abdominal tissue as a pedicled TRAM flap, including the muscle, but this is completely disconnected from the donor site.
TUG (Transverse Upper Gracilis) flap uses skin, fat and muscle from the upper thigh to reconstruct the breast. It is less commonly performed than other procedures, but may be used for women who are not suited to other autologous procedures, but who do not want implant reconstruction.
Gluteal flaps use tissue from the buttocks. It is rarely used but may be an option in limited circumstances.
Pedicled flaps
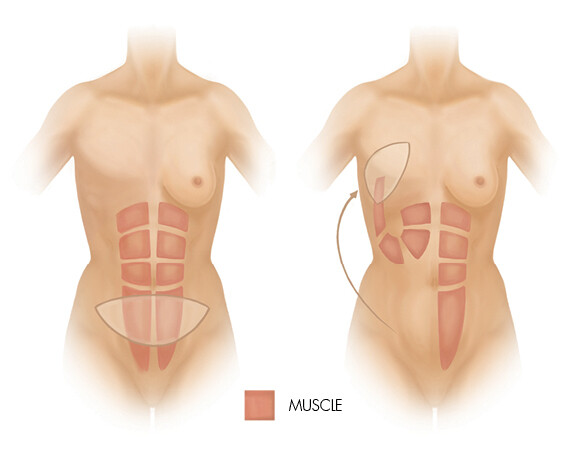
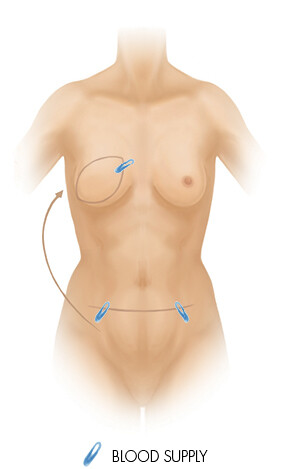
Breast reconstruction with pedicled flaps involves the transfer of skin, fat and muscle to the breast area on a pedicle of muscle that retains the blood supply.
This procedure transfers skin, fat and part of the vertical abdominal muscle to the breast under the abdomen. Abdominal skin is used to fill in the defect on the central part of the breast, while the remaining tissue creates breast volume. The abdomen is flatter after tissue removal, and the navel is repositioned, resulting in a ‘tummy tuck’.
The DIEP flap is now more commonly performed than TRAM flap reconstruction.
Latissimus dorsi flap reconstruction
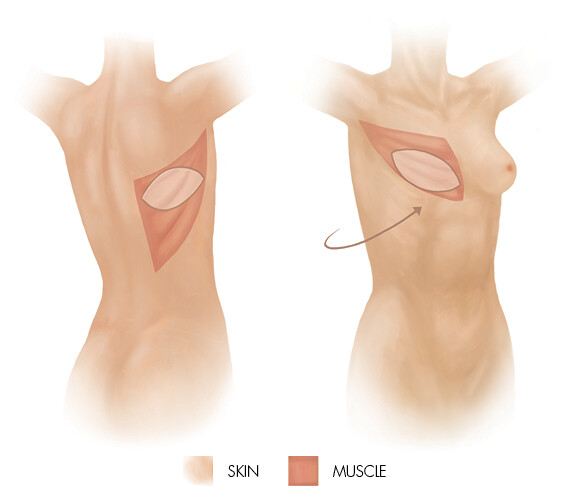
This procedure is better suited to women with small- to medium-sized breasts, and those who wish to avoid TRAM or DIEP flap reconstruction. It may also be used for women who have scarring from previous abdominal surgery or unsuitable abdominal tissue, or who have a previous failed reconstruction.
Women who are planning for future pregnancy may also be suited to this procedure. The procedure uses the latissimus dorsi muscle, fat and skin from the back, which is transferred under the skin to the chest, with the blood supply intact. An implant is commonly used to supplement the breast mound volume. An extended latissimus dorsi flap can be performed, to transfer more fat tissue. Latissimus dorsi flaps are not suited for active sportspeople, as the removal of the muscle from the back may reduce the ability to perform strenuous overhead activities.
Other reconstructions
Microvascular flaps
This procedure completely detaches the skin, fat and some blood vessels from the donor site and, once transferred to the breast area, the blood supply is re-attached through microsurgery.
Perforator flaps
ThoracoDorsal Artery Perforator (TDAP) flap and Lateral InterCostal Artery (LiCAP) flap are recent advances in microsurgery, used to repair defects in the breast after breast-conserving surgery (e.g. lumpectomy, partial mastectomy). However, these procedures are rarely an option.