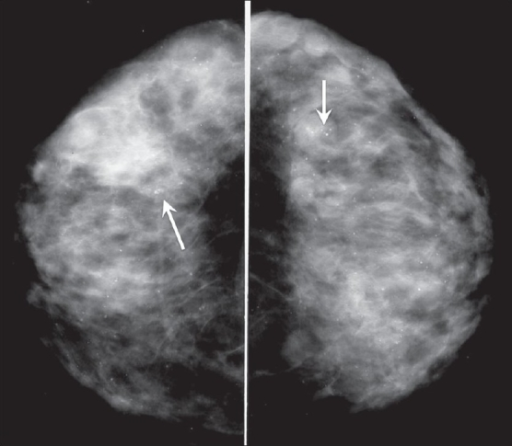
Benign breast calcification
Calcifications occur when there are deposits of calcium in the breast tissue, these small deposits are asymptomatic and are detected on mammogram. They occur in women over 50 years of age, due to the natural ageing of the breast tissue, but can result from previous infection, trauma or surgery, cysts or fibroadenomas, or prior radiation therapy. In some cases, the presence of calcifications can indicate breast cancer. Calcifications that are classified as ‘indeterminate’ will need further testing to exclude cancer.
Duct Ectasia
As the breasts age (from 35 onwards), the ducts behind the nipple shorten and widen, producing nipple discharge. This can be thick or watery, green, black or occasionally blood-stained. A lump may also be felt behind the nipple as tissue thickens and becomes scarred. The nipple may begin to retract as the ducts shorten. Further investigation is required to exclude cancer.
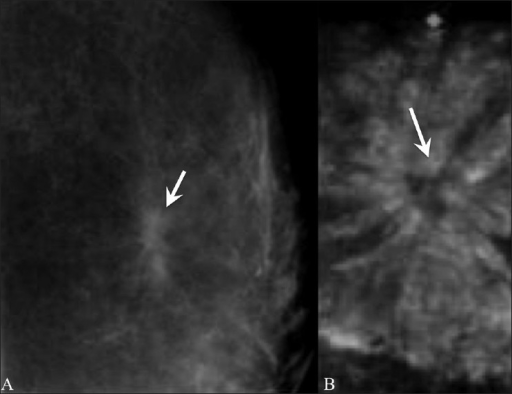
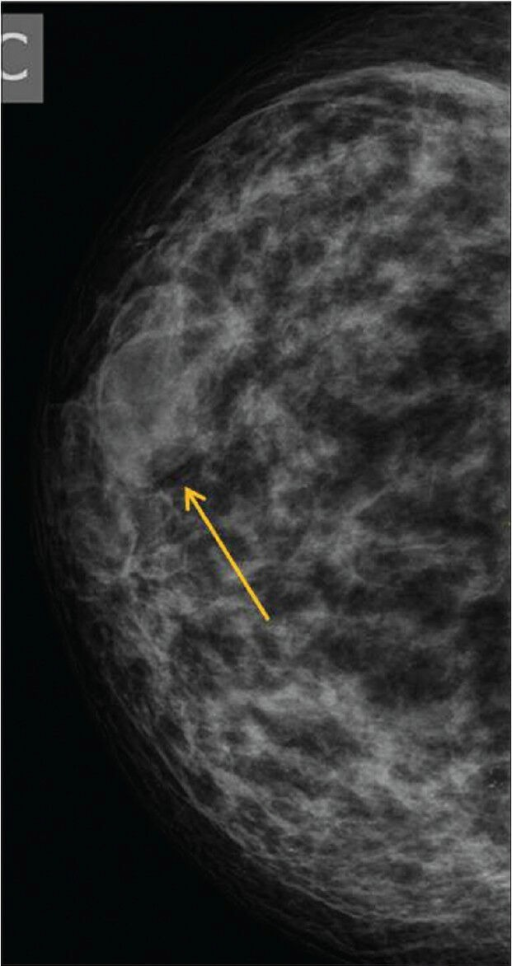
Radial Scar
Radial scars (complex sclerosing lesions) are hardened areas of breast tissue surrounded by abnormal ducts and tissue structures. Most radial scars are found on mammograms. As they resemble cancer, they require core biopsy for testing. Surgical excision is often recommended to confirm the surrounding tissue is normal. A referral to a breast surgeon is required for further investigation.
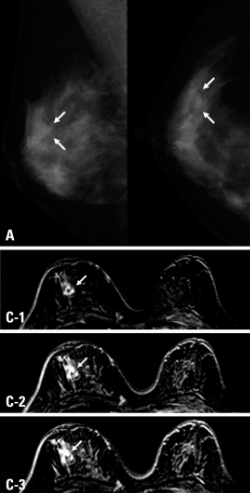
Sclerosing adenosis
This condition is caused by an overgrowth of tissue in the breast lobules. As with radial scars, sclerosing adenosis is generally found on mammogram, as the person will be asymptomatic. It resembles cancer on mammogram and will require further investigation. No treatment is required, but the condition is associated with an increased risk for developing breast cancer.
Intraductal papilloma
This condition, also called papillary neoplasm, is a wart-like growth that develops inside a breast duct near the nipple. Usually detected on mammogram, or patient may present with a lump or nipple discharge. It is most common in women aged 35-55. Further testing is required to exclude breast cancer. Single papillomas with no abnormalities do not increase a women’s risk of breast cancer, but those with papillomatosis (multiple papillomas) have a slightly elevated risk. Regular surveillance is advised for this cohort.
Fat Necrosis
Fat necrosis is caused by damage to fat cells, typically from direct trauma (e.g. seatbelt injury, biopsy, breast surgery such as implant removal or reconstruction). Radiation therapy and anti-coagulants may also cause fat necrosis to develop. Fat necrosis may be felt as a lump, otherwise it is detected via mammogram or ultrasound. They can resemble breast cancer on mammogram, so a biopsy may be needed to exclude malignancy. Usually fat necrosis will resolve on its own without treatment.
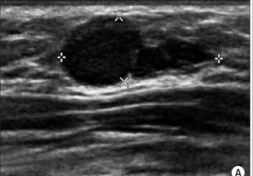
Fibroadenomas
Fibroadenomas usually present as a lump or a change detected on ultrasound/mammogram. Fibroadenomas can vary in size, with some women having more than one. Diagnosis is by core biopsy.
Fibroadenomas are common and thought to be related to estrogen. Although they can appear at any age, they are more likely when aged 15-40 years.
Fibromas are found in the breast lobule and fibrous tissue. Fibroadenomas occurs when tissue in the lobule overgrows and becomes hard.
Most will shrink over time, so are usually left alone. If a fibroadenoma becomes larger or is painful referral to a breast specialist should be made regarding excision.